John (64)July 2015
I can never thank you properly for the amazing help and support that you gave me… Your straight forward – say it as it is; but with a positive and thoughtful approach has made my situation so much easier and less worrying… When I saw my wonderful old GP he asked me who performed my operation and when I told him he smiled and said John, you are a lucky man – you had the best. So Christopher from the bottom of my heart a huge huge thank you for everything that you have done for me with your amazing team and your totally professional, totally dedicated and kind self… You have helped me more than you realise and I am incredibly grateful to you.
The da Vinci® System is a sophisticated robotic platform designed to expand the surgeon’s capabilities – and for the first time – offer minimally invasive option for major surgery.
With the da Vinci®, small incisions are used to introduce miniaturised wristed instruments and a high definition 3D camera. seated comfortably at the da Vinci® console, your surgeon views a magnified, high-resolution 3D image of the surgical site.
At the same time, state-of-the-art robotic and computer technologies scale, filter and seamlessly translate your surgeon’s hand movements into precise micro-movements of the da Vinci® instruments.
The system cannot be programmed, nor can it make decisions on its own. Rather, the da Vinci® System requires that every surgical manoeuvre be performed with direct input from your surgeon.
While clinical studies support the effectiveness of the da Vinci® System when used in minimally invasive surgery, individual results may vary. Surgery with the da Vinci® Surgical System may not be appropriate for every individual. Always ask your doctor about all treatment options, as well as their risks and benefits.
Surgical robotics was little more than a medical curiosity until 1999, the year Intuitive Surgical introduced the da Vinci® Surgical System. Today, Intuitive Surgical is the global leader in the rapidly emerging field of robotic-assisted minimally invasive surgery. Since its inception, the company has consistently provided surgeons and hospitals with the tools needed to improve clinical outcomes and to help patients return to active and productive lives.
With its corporate headquarters located in Sunnyvale California, Intuitive Surgical serves customers throughout the United States and internationally, providing technology and procedural innovation across cardiac, urology, gynecologic, peadiatric and general surgical disciplines.
Robotic Assisted Da Vinci® Radical Prostatectomy
Surgery to remove the prostate gland is one of the ways of treating early or localised prostate cancer. Active surveillance, brachytherapy and external beam radiotherapy are all alternative treatments for early or localised prostate cancer. Your doctor should discuss with you which options are suitable for you.
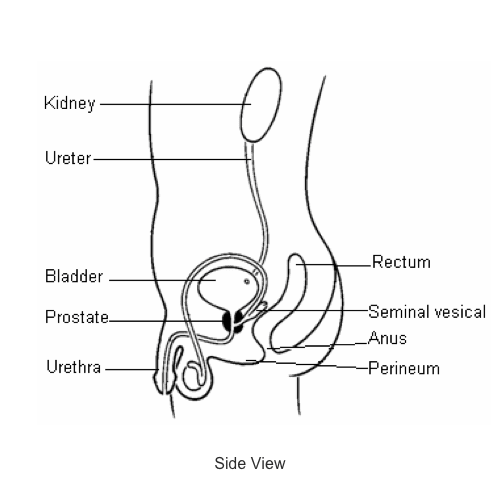
A radial prostatectomy is an operation performed by a specialist surgeon, it involves the removal of the prostate, seminal vesicles and surrounding tissues. Lymph nodes that are part of the lymphatic system which normally helps fight infection or disease may also be removed during this operation. Radical prostatectomy may be performed in several different ways.
- Open retropubic (through an abdominal incision) prostatectomy
- Perineal prostatectomy (through an incision in the area between the testicles and back passage) Laparoscopic (Keyhole)
- Standard approach (by hand)
- Robotic assisted (Da Vinci®)

What is robotic assisted (Da Vinci®) prostatectomy?
The Da Vinci® prostatectomy operation involves the removal of the prostate and the seminal vesicles (two small glands behind the prostate). The bladder is then rejoined to the urethra (the water pipe which runs through the penis).
The procedure is carried out under general anaesthetic and you will, therefore, be asleep throughout the operation. The surgeon will make small “keyhole” or “port” incisions through which a camera and instruments are inserted. Six ports are needed for a radical prostatectomy; one for a high-magnification 3D camera to allow the surgeon to see inside your abdomen, the others are for instruments.
The instruments are approximately 7mm wide and are designed to move in a similar way to the human hand and wrist. In fact they have a greater range of movement than the human hand, enabling the surgeon to carry out the operation in a small space.
In the operating theatre a robotic console with four robotic arms will be placed beside you. Three arms are for instruments and one is for the high-magnification 3D camera. The surgeon performing the operation sits at a console which is in the same room but away from the operating table.
The console contains master controls which the surgeon uses to manipulate the instruments inside the patient. The robot cannot work on its’ own.
The length of time taken to perform the surgery is usually between three to four hours. Recovery afterwards is usually quicker than in open surgery. Your fitness for such an operation will be assessed and discussed by your Urologist.
The Urologist will discuss the details of the procedure with you during your outpatient appointment. You should be aware that there is a small chance your procedure may need to be converted to an open procedure.
If for any reason you would not agree to an open operation under any circumstances, we would be unable to go ahead with the robotic operation.
What happens before the procedure?
Before the prostatectomy you will be asked to attend the hospital to make sure you are fit for the anaesthetic .This is called a pre-assessment visit. This appointment can take three – four hours.
Chris (64)November 2014July 2015
I would like to express my great gratitude to you for your obviously excellent judgement and surgical skill which resulted in both a quick recovery with negligible pain and finally the most satisfactory outcome.
Ian (70)June 2015
The care from Mr Ogden has been outstanding and I am eternally grateful to him.
During this appointment you will meet a Pre- Assessment Nurse who will undertake the following:
- A history of your current and past health concerns or problems including any medication you may be taking
- A physical examination
- Blood tests
- MRSA screen (to find out if you are a carrier of MRSA). You may have had this done at a clinic visit so this will not need to be repeated.
- ECG (electrocardiogram ) to check heart rhythm
- Observations including blood pressure, temperature, pulse height, weight and abdominal girth measurement. In order to perform the surgery your weight must be below 100kg and abdominal girth is less than 40 inches. This makes surgery easier and you will have a better recovery. If your weight or girth measurements are too great then we may need to postpone surgery. If you require any information about healthy eating and exercise, then please speak with the pre- assessment nurse.
- Referral for other tests if required.
You may also meet the Uro-Oncology Clinical Nurse Specialist (CNS) who will recap the details of your surgery and will discuss what to expect after your operation. You will also be shown some of the equipment you will use after the operation for example a urinary catheter, drainage bags, and support straps. You will have an opportunity to ask questions.
An anaesthetist who will ask you about your past and current health concerns as well as what medicines you are taking. If you have had a history of heart or breathing problems the anaesthetist may refer you for further tests. This is to check that you are fit for an anaesthetic. You will be able to ask the anaesthetist any questions about your anaesthetic or pain control after the operation. A member of the surgical team will fully discuss the aims, extent of the surgery and potential risks of the procedure. This explanation is essential to help you make an informed decision and sign a consent form agreeing to surgery.
It would be helpful if you could bring the following information to your pre-admission appointment:
GP address and phone and fax number – so that we can keep your GP fully informed of your treatment and recovery.
Community nurse’s address, phone and fax number – when you go home, we will refer you to the community nurses to provide you with additional home support for about one week. The community nurses are often based at your GP surgery.
If after surgery you are NOT going home to your current address you will have to register as a temporary resident with the GP of the family/friends you will be staying with. This is so that you can have access to the Community Nurses covering that area. We will need the contact details of your temporary GP and community nurse team.
If you do not meet everyone on your pre-assessment visit you will meet them when you come into hospital for your operation.
Please ask if you are not happy with something, or do not understand what is being said.
Transport
You will need to consider how you will get to and from the hospital. You will need to be at the hospital at 7am for same-day surgery. There are no parking facilities in this hospital. If you are travelling by public transport then please check the times of your trains/buses/tubes to ensure that you can arrive on time. If you are going home by public transport, please make sure you have someone to go home with you as you will not be able to lift any heavy objects for six weeks.
Hospital transport is only provided on exceptional medical grounds. Please tell the pre-admission team if you think you may have transport problems.
Are there any side-effects of the surgery?
Common side-effects - 1 in 10 patients
- Temporary insertion of a bladder catheter
- Temporary difficulties with urinary control
- Impairment of erections due to unavoidable nerve damage (20-50% of men with good pre-operative sexual function)
- Inability to ejaculate or father children because the structures which produce seminal fluid have been removed (occurs in 100% of patients)
- The discovery that cancer cells have already spread outside the prostate requiring further treatment
Occasional side-effects- between 1 in 10 & 1 in 50 patients
- Temporary insertion of a bladder catheter
- Temporary difficulties with urinary control
- Impairment of erections due to unavoidable nerve damage (20-50% of men with good pre-operative sexual function)
- Inability to ejaculate or father children because the structures which produce seminal fluid have been removed (occurs in 100% of patients)
- The discovery that cancer cells have already spread outside the prostate requiring further treatment
Rare side-effects - less than 1 in 50 patients
- Temporary insertion of a bladder catheter
- Temporary difficulties with urinary control
- Impairment of erections due to unavoidable nerve damage (20-50% of men with good pre-operative sexual function)
- Inability to ejaculate or father children because the structures which produce seminal fluid have been removed (occurs in 100% of patients)
- The discovery that cancer cells have already spread outside the prostate requiring further treatment
Michael (80) June 2015
Nine and a half years is indeed a long time and I thought I owed it to you to say thank you for what was then, I know, an experimental procedure and which still apparently has done the trick. So this is just to say thank you.
Contact details
If you have any further questions after reading this information, please contact your consultants or your uro-oncology nurse specialist on the numbers listed below.
Consultant: 0207 352 8171 and ask to be put through to consultant office
Clinical Nurse Specialist (your key worker): Amanda Baxter 0207 808 2817
Transitional Care Unit: 0207 808 2405/2406